SYMPTOMS OF SICKLE CELL DISEASE
The symptoms of SCD are typically intermittent, meaning they are experienced in episodes that come and go. Symptoms also tend to vary in frequency and severity from person to person and may change over time. They can occur in conditions that cause hypoxia (low oxygen), such as intense physical exertion or stress, infections including malaria, cold and dehydration. Symptoms of SCD may include:
* Painful episodes
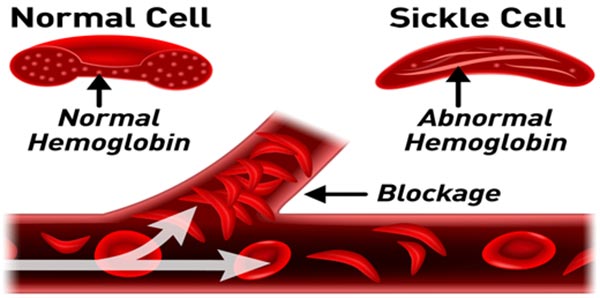
Episodes of pain – also known as sickle cell crises (e.g vaso-occlusive crisis) – are one of the most common symptoms of SCD. The pain can vary in severity and may come on suddenly. Most often it is felt in the bones and joints, though it may also occur in other locations, such as the hands, feet, arms, legs or abdomen. Any area with both sensory nerves and blood supply can be affected during a painful episode. Many people with SCD experience chronic, low-level pain, often in bones and joints. Painful episodes are caused by sickle-shaped cells blocking blood vessels and cutting off the oxygen supply to tissues. Unlike normal red cells, which are usually smooth and malleable, the sickle red cells cannot squeeze through small blood vessels. When the sickle cells block small blood vessels, the organs are deprived of blood and oxygen. This leads to periodic episodes of pain and damage the vital organs. Sickle red cells die after only about 10 to 20 days instead of the usual 120 days, because they cannot be replaced fast enough the blood is chronically short of red cells, causing anemia.
Type of sickle cell crisis include:
- Vaso-occlusive crisis (VOC)
- Visceral sequestration crisis
- Acute abdominal crisis
- Aplastic crisis
* Acute chest syndrome
Acute chest syndrome occurs when blood vessels in the lungs become blocked, typically causing chest pain, a high temperature, coughing and shortness of breath. It is treated as a medical emergency requiring urgent treatment.
* Infections
People with SCD are susceptible to severe infection from certain types of bacteria. Common types of infection include: blood infection, also known as septicemia lung infection, also known as pneumonia, infection of the surroundings of the brain and the spine, also known as bacterial meningitis, bone infection, also known as osteomyelitis and malaria infection.
* Severe anemia
People with SCD will normally also experience mild to moderate anemia, a lack of hemoglobin. Periodically, however, this anemia can become severe and require urgent medical attention. This may occur suddenly or more gradually. Signs and symptoms of the onset of severe anemia include: Tiredness, Shortness of breath, Dizziness, Nausea, Paleness, particularly in the eyelids, lips, tongue and nail beds.
*Jaundice (yellowness of the eyes)
This occurs as a result of lysis of the sickled (crescent shaped) red blood cells with a resultant yellow pigment called bilirubin which is responsible for the yellow coloration of the eyes, the mucous membrane of the mouth, the Palm, the sole of the feet and the nail beds.
Abdominal protrusion
In individuals whose spleen has not gone through auto-splenectomy (self-shrinkage) before the age of six (6) years, the enlargement of the spleen makes the abdomen big. If the liver is equally enlarged, these two organs are responsible for the abdominal protrusion that is seen in some of them.
Hypognatism and frontal bossing
Under development of the jaw results in this and it is seen in most sickle cell disease individuals. Bossing of the frontal part of the head is referred to as frontal bossing, this is also common in SCD.
MANAGEMENT OF SICKLE CELL DISEASE
A number of treatment methods are available to manage the symptoms of SCD and prevent complications. However, in most cases, the disorder cannot be cured and will require lifelong management. Individuals with sickle-cell disease are placed on routine medications which includes multivitamins like folic acid, vitamin Bco, multivite, vitamin c, they are also expected to use malaria preventive either Paludrine tablets which is taken on daily basis or metaprim tablets which is taking once a week. Iron supplements should be avoided as it is injurious to their health, they have more than enough iron from the broken down red cells. Liberal oral fluid intake should be taken generously, at least about 5 liters of water per day. They should practise good personal hygiene, eat balanced healthy diet and avoid precipitating factors that will cause sickle cell crisis such as cold, stress, infection and extreme physical exertion.
People with SCD are managed by medical Doctors and will be required to attend check-ups at regular intervals. They will also be taught how to recognise the condition’s symptoms, so that treatment can be given as soon as possible after they appear. Staying healthy is an important principle of managing SCD.
Goals of SCD management include maximizing tissue oxygenation (perfusion), preventing and treating complications associated with anemia and sickle-cell crisis, preventing and aggressively treating infection including malaria and other blood borne infections, and managing pain.
If a painful episode is severe, professional medical attention should be sought as soon as possible. If fever appears, medical attention should be sought right away: fever is a medical emergency in people with SCD.
Oral hydroxyurea (HU)
Long-term oral hydroxyurea (HU) administration reduces or prevents many acute and chronic complications of SCD. HU is rapidly absorbed, has near-complete bioavailability, and is therapeutic with once-daily oral dosing. Decades of research have established that the most effective treatment for SCD is to increase circulating normal or fetal hemoglobin (HBF) and reduce HBSS. Increasing the concentration of HBF is the primary effect of HU. Other benefits of HU include lowering the number of circulating leukocytes (white blood cells) and reticulocytes (immature red blood cells) and decreasing their adhesiveness, which can reduce vascular occlusion leading to VOC. HU also increases RBC size and improves cellular deformability, which increases blood flow and reduces VOC. Nitric oxide, a vasodilator, is released directly from HU metabolism and may contribute to local vasodilation.
HU therapy substantially reduces the frequency of painful episodes associated with VOC and the need for transfusions and hospitalizations. Indications for HU therapy include recurrent VOC (3 or more severe episodes requiring admission in the last 12 months), recurrent acute chest syndrome (2 or more episodes in a lifetime), severe symptomatic anaemia, and recurrent priapism (unnessary painful erection). Although HU isn’t as effective as blood transfusion therapy in preventing stroke or VOC, it’s the most widely used therapy and has proven efficacy in children and adults with SCD. HU is the only FDA-approved pharmacologic treatment for induction of HbF in adults with SCD, and it’s also approved by the European Medicines Agency for both children and adults with SCD. The benefit is directly related to the amount of HbF produced in response to the drug. However, several clinical studies have shown that individual responses to HU treatment vary.
… To be continued
Related News